Background
Cisplatin-based NAC is considered as standard of care for NM-MIBC pts based on a modest survival benefit correlated with pathological complete response (pCR). Avelumab, a monoclonal antibody directed against PD-L1, showed efficacy in advanced urothelial cancer. We report preliminary data from the AURA trial assessing preoperative avelumab associated with two cisplatin-based regimens in the cisplatin eligible cohort.
Methods
AURA is a prospective, multicenter, randomized, phase II trial for pts with cT2-4aN0-2M0 bladder carcinoma. Cisplatin-eligible pts received cisplatin-gemcitabine (CG) plus A or dose-dense MVAC (DD-MVAC) plus A (1:1). Primary endpoint was pCR (ypT0/isN0) with the objective, in each arm, to show pCR rate > 25% (90% power reached in case of pCR rate > 45%). Two-step design was used with planned interim analysis after 28 evaluable pts per arm. Secondary endpoints were pathologic downstaging rate (
Results
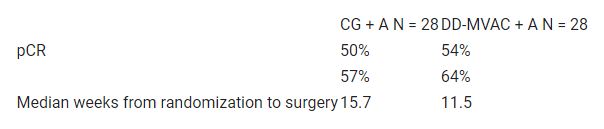
At interim analysis data cut-off, 56 cisplatin-eligible pts were evaluable. For CG + A arm (n=28): median age was 69 years (41-81), 64% male, 7% cT4 and 7% cN+. For DD-MVAC + A arm (n=28): median age was 62 years (51-77), 79% male, 7% cT4 and 7% cN+. Six pts did not undergo surgery but were included in intention to treat analysis. Efficacy outcomes according to treatment regimen are represented in the table. Most common grade 3/4 AEs were thrombocytopenia (29%), acute kidney injury (18%) neutropenia (14%), and anemia (13%). No patients required steroids for immune-related AEs. No treatment-related deaths were reported. The IDMC recommended stopping accrual in this cohort because the endpoint was reached.
Conclusions
Interim results from the AURA phase II trial demonstrate a high pCR rate with neoadjuvant avelumab in combination with each cisplatin-based NAC regimen. Further results in cisplatin eligible/ineligible cohorts and correlative studies will be presented.
Clinical trial identification
NCT03674424.
Editorial acknowledgement
Legal entity responsible for the study
CTSU – Jules Bordet Institute.
Funding
Merck N.V.-S.A., Belgium, an affiliate of Merck KGaA, Darmstadt, Germany, as part of an alliance between Merck KGaA and Pfizer.
Disclosure
All authors have declared no conflicts of interest.